What Does It Mean When a Baby Projectile Vomits
Contents
- What is projectile vomiting
- Projectile vomiting in infants
- Pyloric stenosis complications
- What are the signs and symptoms of pyloric stenosis?
- What causes pyloric stenosis?
- Chance factors for pyloric stenosis
- How is pyloric stenosis diagnosed?
- Pyloric stenosis treatment
- Projectile vomiting in adults
- What causes projectile vomiting in adults
- Projectile vomiting in adults diagnosis
- Projectile vomiting in infants
What is projectile vomiting
Projectile airsickness simply means forced airsickness frequently occurring suddenly and without alarm, i.e. without nausea and retching. Consequently an individual may have an episode of projectile airsickness at whatever time, due east.m. while standing in a queue, on public ship, or in a restaurant or hospital bed.
Effigy ane. Breadbasket
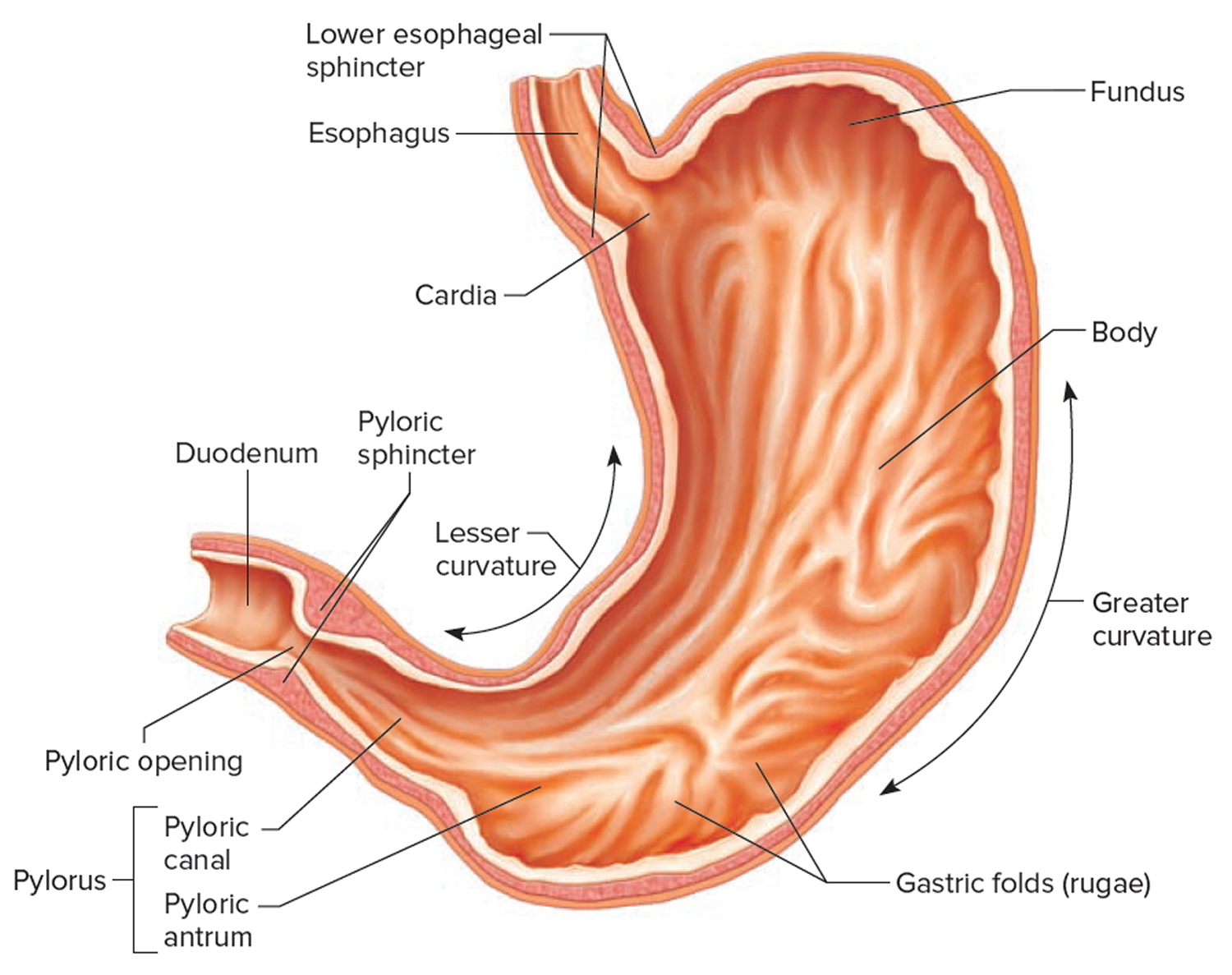
Effigy 2. Parts of the stomach
Projectile vomiting in infants
Pyloric stenosis is an uncommon condition in infants that blocks nutrient from entering the small intestine. Normally, nutrient and other stomach contents pass through the pylorus, the lower part of the stomach, to enter the pocket-sized intestine. A muscular valve (pyloric sphincter) between the stomach and pocket-sized intestine holds food in the tum until it is set up for the next stage in the digestive process. In pyloric stenosis, the pylorus muscles thicken and become abnormally large, blocking food from reaching the small intestine and prevents food from elimination out of the stomach.
Pyloric stenosis besides called infantile hypertrophic pyloric stenosis, is a type of gastric outlet obstruction, which means a blockage from the stomach to the intestines, can lead to projectile vomiting, aridity and weight loss. Babies with pyloric stenosis may seem to exist hungry all the time.
Signs and symptoms of pyloric stenosis include:
- Airsickness after feeding. The baby may vomit forcefully, ejecting breast milk or formula up to several feet abroad (projectile airsickness). Vomiting might be mild at showtime and gradually get more severe equally the pylorus opening narrows. The vomit may sometimes comprise blood.
- Persistent hunger. Babies who take pyloric stenosis oft desire to eat presently subsequently vomiting.
- Stomach contractions. You may notice wave-like contractions (peristalsis) that ripple across your infant's upper abdomen before long after feeding, but before vomiting. This is acquired by stomach muscles trying to force food through the narrowed pylorus.
- Dehydration. Your baby might weep without tears or go lethargic. You might find yourself changing fewer wet diapers or diapers that aren't as moisture equally you expect.
- Changes in bowel movements. Since pyloric stenosis prevents food from reaching the intestines, babies with this condition might be constipated.
- Weight issues. Pyloric stenosis can keep a baby from gaining weight, and sometimes can cause weight loss.
Pyloric stenosis affects about 3 out of 1,000 babies in the United States. Information technology's more probable to affect firstborn male person infants and as well runs in families — if a parent had pyloric stenosis, then a baby has up to a 20% adventure of developing it. Most infants who have pyloric stenosis develop symptoms iii to 5 weeks after nascency.
Pyloric stenosis needs firsthand medical treatment and surgery cures pyloric stenosis.
Key points
- Correction of fluid deficit, electrolyte and acid base abnormalities is the priority
- Following fluid resuscitation (if required) 0.ix% Sodium Chloride with five% glucose and 20mmol/l Potassium Chloride should be used for replacement of arrears and ongoing fluid maintenance.
- Surgical correction may be safely delayed until correction of fluid deficit, electrolyte and acid base abnormalities.
When to run across a doctor
Pyloric stenosis is an urgent condition that needs immediate treatment.
Meet your doctor if your baby:
- has lasting or projectile vomiting afterwards feeding
- is losing weight or non gaining weight as expected
- is less active than usual or is very sleepy
- has few or no stools (poops) over a flow of i or 2 days
- show signs of dehydration, such as more than iv to 6 hours between wet diapers, a sunken "soft spot" on the head, or sunken eyes
Pyloric stenosis complications
Pyloric stenosis can atomic number 82 to:
- Failure to grow and develop.
- Dehydration. Frequent airsickness tin cause dehydration and a mineral (electrolyte) imbalance. Electrolytes help regulate many vital functions.
- Tummy irritation. Repeated vomiting can irritate your babe's tummy and may cause mild bleeding.
- Jaundice. Rarely, a substance secreted by the liver (bilirubin) tin can build up, causing a yellowish discoloration of the peel and eyes.
What are the signs and symptoms of pyloric stenosis?
Symptoms of pyloric stenosis typically begin when a baby is around iii weeks sometime. They include:
- Vomiting. The first symptom is usually airsickness. At starting time it may seem that the baby is just spitting up oft, only then it tends to become projectile airsickness, in which the breast milk or formula is ejected forcefully from the rima oris, in an arc, sometimes over a altitude of several feet. Projectile vomiting usually takes identify presently afterward the cease of a feeding, although in some cases it can happen hours afterwards. The vomited milk might olfactory property curdled because it has mixed with stomach acid. The vomit will non incorporate bile, a green fluid from the liver that mixes with digested food after it leaves the stomach. Despite vomiting, a babe with pyloric stenosis is usually hungry over again soon after vomiting and volition want to eat. It'due south important to know that even with the airsickness, the baby might non seem to be in dandy hurting or at first await very ill.
- Changes in stools. Babies with pyloric stenosis usually take fewer, smaller stools (poops) considering fiddling or no food is reaching the intestines. Constipation or poop with mucus too can happen.
- Failure to gain weight or weight loss. Most babies with pyloric stenosis will fail to gain weight or will lose weight. Equally the condition gets worse, they might become dehydrated.
- Dehydrated infants are less active than usual, and they may develop a sunken "soft spot" on their heads and sunken eyes, and their skin may look wrinkled. Considering less pee is made, they can go more than than 4 to 6 hours between wet diapers.
- Waves of peristalsis. After feeds, increased stomach contractions may make noticeable ripples, which move from left to right over the baby'south belly as the stomach tries to empty itself against the thickened pylorus.
It'south important to see your doctor if your babe has whatever of these symptoms.
Other conditions tin can cause like issues. For instance:
- Gastroesophageal reflux (GER) usually begins before 8 weeks of age. Gastroesophageal reflux involves lots of spitting upwards (reflux) after feedings, which tin look similar vomiting. But most babies with gastroesophageal reflux don't accept projectile vomiting, and while they might take trouble gaining weight, they normally accept normal poops.
- A milk poly peptide allergy also can make a baby spit up or vomit, and have diarrhea. But these babies don't have projectile vomiting.
- Gastroenteritis (inflammation in the digestive tract that can exist caused by viral or bacterial infection) also can cause vomiting and aridity. But babies with gastroenteritis unremarkably also have diarrhea with loose, watery, or sometimes bloody stools. Diarrhea usually isn't seen with pyloric stenosis.
What causes pyloric stenosis?
It's thought that babies who develop pyloric stenosis are non born with it, but have progressive thickening of the pylorus after nascence. A baby will start to show symptoms when the pylorus is so thick that the stomach tin't empty properly.
The cause of this thickening isn't articulate. Information technology might exist a combination of several things; for example, utilize of erythromycin (an antibiotic) in babies in the kickoff 2 weeks of life or antibiotics given to moms at the stop of pregnancy or during breastfeeding can be associated with pyloric stenosis.
Take chances factors for pyloric stenosis
Risk factors for pyloric stenosis include:
- Sex. Pyloric stenosis is seen more often in boys — especially firstborn children — than in girls.
- Race. Pyloric stenosis is more common in Caucasians of northern European ancestry, less common in African-Americans and rare in Asians.
- Premature birth. Pyloric stenosis is more common in babies born prematurely than in full-term babies.
- Family unit history. Studies found higher rates of this disorder among certain families. Pyloric stenosis develops in virtually 20 percent of male descendants and 10 percent of female descendants of mothers who had the condition.
- Smoking during pregnancy. This beliefs tin nearly double the gamble of pyloric stenosis.
- Early on antibiotic utilise. Babies given certain antibiotics in the first weeks of life — erythromycin to treat whooping cough, for instance — have an increased risk of pyloric stenosis. In improver, babies born to mothers who took certain antibiotics in late pregnancy also may have an increased chance of pyloric stenosis.
- Bottle-feeding. Some studies suggest that bottle-feeding rather than breast-feeding can increase the risk of pyloric stenosis. Nigh people in these studies used formula rather than breast milk, then information technology isn't articulate whether the increased run a risk is related to formula or the mechanism of bottle-feeding.
How is pyloric stenosis diagnosed?
The doctor will ask detailed questions about the baby's feeding and vomiting patterns, including what the vomit looks similar. The infant volition be examined, and any weight loss or failure to maintain growth since birth will be noted.
The doctor will cheque for a lump in the abdomen, which usually is house and movable and feels like an olive. If the dr. feels this lump, information technology'southward a strong indication that a baby has pyloric stenosis.
Visible gastric peristalsis (may be more obvious post-obit a feed).
Pyloric mass:
- Located at the lateral edge of the rectus abdominis muscle in the correct upper quadrant
- Best felt from the left side with the infant settled and supine.
- May be difficult to palpate. May require repeated examinations or to expect for several minutes with hand on abdomen to experience.
When pyloric stenosis seems likely, an intestinal ultrasound ordinarily is done. The enlarged, thickened pylorus tin can be seen on ultrasound images. The doc may ask that the babe not be fed for several hours earlier an ultrasound.
Sometimes a barium swallow is done instead of an ultrasound. Babies consume a small amount of a chalky liquid (barium), and then special 10-rays are taken to view the pyloric area of the stomach to see if there is whatever narrowing or blockage.
The doctor also might order blood tests to bank check levels of electrolytes (minerals that help keep fluids balanced and vital organs working properly). An electrolyte imbalance often happens due to the ongoing vomiting of stomach acrid and dehydration, and needs to exist corrected.
Pyloric stenosis treatment
When an infant is diagnosed with pyloric stenosis, either by ultrasound or barium swallow, the babe will be admitted to the hospital and prepared for surgery. Whatsoever dehydration or electrolyte problems in the claret will be corrected with intravenous (4) fluids, unremarkably within 24 hours.
- Surgical correction of hypertrophic pyloric stenosis is usually delayed until correction of acid/base condition, electrolyte disturbances and dehydration.
- Information technology is particularly important to fully correct serum bicarbonate earlier surgery because of the risk of hypoventilation/apnoea mail service-operatively in the setting of a metabolic alkalosis.
A surgical procedure called pyloromyotomy, which involves cutting through the thickened muscles of the pylorus, volition salve the blockage. The pylorus is examined through a very minor incision, and the muscles that are overgrown and thickened are spread and relaxed.
The surgery tin also be done through laparoscopy. This is a technique that uses a tiny scope placed in an incision in the belly button, allowing the doctor to see the area of the pylorus. Using other small instruments placed in nearby incisions, the physician can consummate the surgery.
Potential complications from pyloric stenosis surgery include bleeding and infection. However, complications aren't common, and the results of surgery are generally first-class.
Most babies render to normal feedings adequately chop-chop, usually 3 to 4 hours later the surgery. Because of swelling at the surgery site, a babe may notwithstanding vomit small amounts for a solar day or so. If there are no complications, most babies who have had pyloromyotomy can render to a normal feeding schedule and get habitation within 24 to 48 hours of the surgery.
If you're breastfeeding, you might worry well-nigh continuing while your infant is hospitalized. The hospital staff should be able to provide a breast pump and help you employ it and so that you lot can continue to express milk until your babe can feed regularly.
Later a successful pyloromyotomy, your baby won't need to follow any special feeding schedules. Your doc will probably want to examine your child at a follow-upwardly appointment to make sure the surgical site is healing properly and that your baby is feeding well and maintaining or gaining weight.
Pyloric stenosis should non happen again after a pyloromyotomy. If your infant still has symptoms weeks afterwards the surgery, there might be another medical trouble, such every bit gastritis or gastroesophageal reflux, so let your doctor know correct away.
Projectile vomiting in adults
Airsickness may be due to a variety of diseases, particularly in the upper gastro-intestinal tract and these include gastric and duodenal ulcers and reflux oesaphagitis. Vomiting may too be a feature of gastro oesophageal reflux disease (GERD). If vomiting occurs soon after swallowing and consists of fresh food at that place may be obstruction in the esophagus. Vomiting may also occur in the older population when dysmotility is present. Vomiting can occur when at that place is obstruction in the small intestine or the colon, the vomitus ordinarily is bile stained and contains fungus and altered food. When the obstruction is lower down in the bowel there may be a odor suggesting feces in the vomit. Medication is another cause of vomiting.
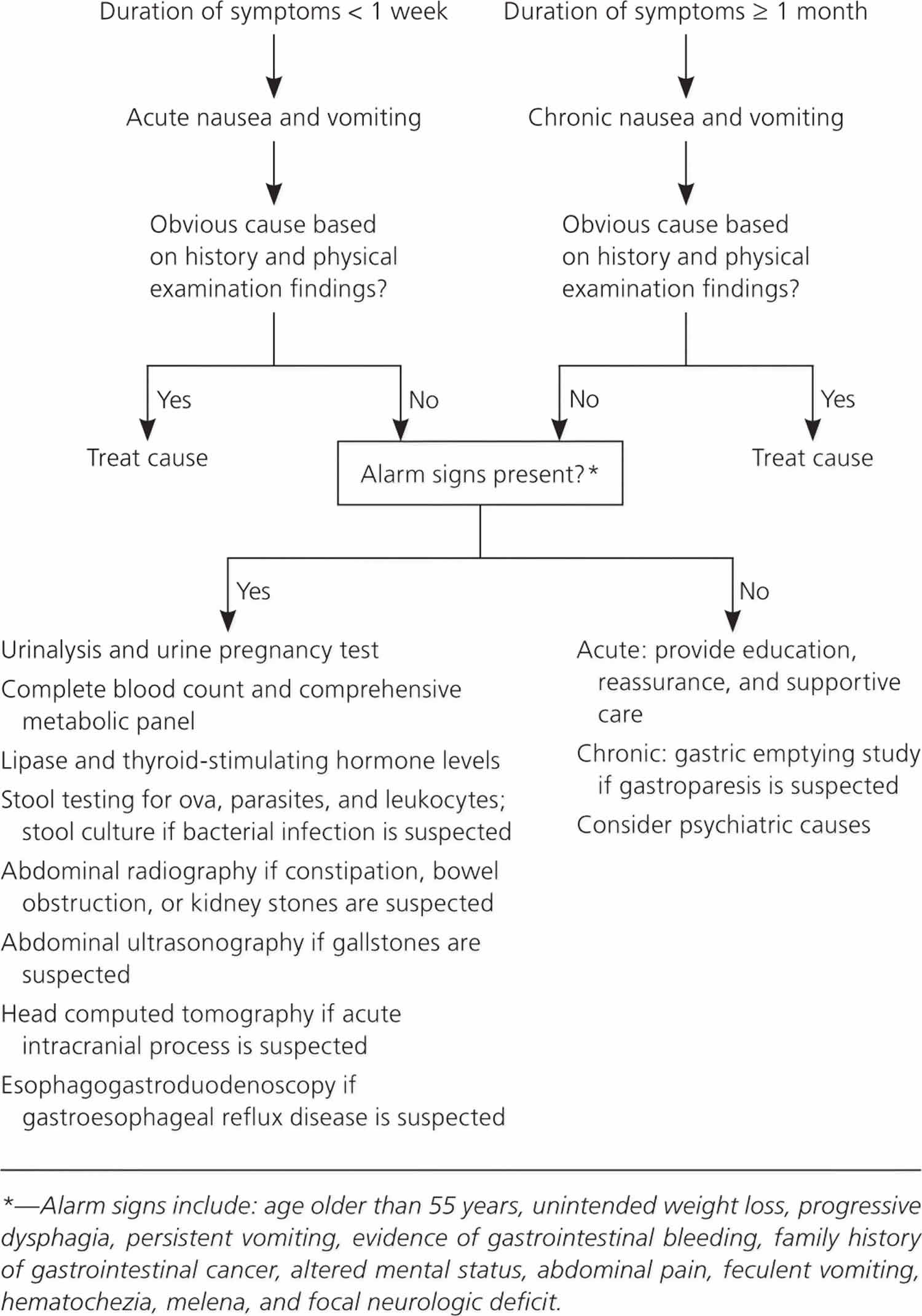
Other potential diagnoses include endocrine atmospheric condition (including pregnancy), central nervous system disorders, psychiatric causes, toxin exposure, metabolic abnormalities, and obstructive or functional gastrointestinal causes. The probable cause of a vomiting can normally be determined by history and concrete exam. Alert signs such as aridity, acidosis acquired by an underlying metabolic disorder, or an acute abdomen warrant boosted evaluation. Based on the suspected diagnosis, basic laboratory testing may include urinalysis, urine pregnancy testing, complete blood count, comprehensive metabolic panel, amylase and lipase levels, thyroid-stimulating hormone level, and stool studies with cultures. Imaging studies include abdominal radiography, ultrasonography, and computed tomography. Computed tomography of the head should be performed if an acute intracranial procedure is suspected. Chronic nausea and airsickness is defined by symptoms that persist for at least one month. Patients with risk factors for gastric malignancies or alarm symptoms should be evaluated with esophagogastroduodenoscopy. If gastroparesis is suspected, a gastric emptying study is recommended. In addition to functional causes, it is as well important to consider psychiatric causes when evaluating patients with chronic nausea and vomiting.
Diagnostic and direction strategies vary depending on the duration of symptoms.
What causes projectile vomiting in adults
Cocky-limited viral gastroenteritis is the well-nigh mutual cause ane) . Approximately 179 million episodes of astute gastroenteritis occur each twelvemonth in the U.s. and effect in roughly 600,000 hospitalizations. Although this illness typically resolves in three to five days, it results in pregnant fourth dimension lost from work and accounts for an estimated $i billion per yr in direct and indirect costs 2) . Only xx% of acute gastroenteritis cases are attributed to a specific etiology three) . Viruses are the almost common cause; norovirus is the well-nigh common in adults.
Mutual and uncommon causes of acute nausea and vomiting in adults 4) :
Cardinal nervous arrangement
- Common
- Benign positional vertigo
- Migraine
- Movement sickness
- Uncommon
- Cerebrovascular result
- Closed caput injury
- Hydrocephalus
- Mass lesion
- Meniere affliction
- Meningitis
- Pseudotumor cerebri
- Seizure disorder
Gastrointestinal
- Common
- Appendicitis
- Cholecystitis
- Cholelithiasis
- Gastritis
- Gastroesophageal reflux disease (GERD)
- Gastroparesis
- Irritable bowel syndrome (IBS)
- Peptic ulcer disease
- Uncommon
- Adhesions
- Esophageal motility disorders
- Incarcerated hernia
- Abdominal obstruction
- Mesenteric ischemia
- Pancreatitis
- Peritonitis
Infections
- Mutual
- Bacterial gastroenteritis
- Foodborne illness
- Pyelonephritis
- Viral gastroenteritis
- Uncommon
- Brain abscess
- Encephalitis
- Meningitis
- Pneumonia
Metabolic
- Common
- Diabetic ketoacidosis
- Pregnancy
- Uremia
- Uncommon
- Adrenal disorders
- Parathyroid disorders
- Thyroid disorders
Medications and toxins
- Antiarrhythmics, antibiotics, anticonvulsants, arsenic, chemotherapeutics, digoxin, estrogens, ethanol overdose, nonsteroidal anti-inflammatory drugs, opiates, organophosphates and pesticides, overdoses and withdrawal, radiation therapy or exposure, ricin
Other
- Acute glaucoma, astute myocardial infarction, nephrolithiasis, pain, psychiatric disorder
[Source 5) ]
Table 1. Nausea and Vomiting That Suggest Specific Diagnoses
| Clinical presentation | Suggested diagnoses | Suggested tests |
|---|---|---|
| Acute onset | Cholecystitis, gastroenteritis, medication-related upshot, pancreatitis | Cholecystitis: right upper-quadrant ultrasonography |
| Pancreatitis: amylase and lipase levels, ultrasonography to assess for gallstones, dissimilarity-enhanced abdominal computed tomography in patients with severe disease | ||
| Associated with diarrhea, headache, and myalgias | Viral gastroenteritis | None |
| Ailing vomiting | Minor bowel obstruction | Abdominal radiography or computed tomography |
| Continuous vomiting | Conversion disorders | Electrolyte levels |
| Delayed vomiting (more than one 60 minutes later meals) | Gastric outlet obstacle, gastroparesis | Obstruction: abdominal radiography |
| Gastroparesis: gastric emptying study | ||
| Feculent or foul aroma to vomitus | Abdominal obstruction | Abdominal radiography |
| Habitual postprandial, irregular vomiting | Major low | Patient Health Questionnaire-9, Beck Low Inventory |
| Insidious onset | Gastroesophageal reflux, gastroparesis, medication-related effect, metabolic disorders, pregnancy | Gastroesophageal reflux: esophagogastroduodenoscopy if patient has alert signs or does not improve with empiric therapy |
| Gastroparesis: gastric emptying study | ||
| Metabolic disorders: pulse oximetry, arterial blood gases, serum chemistries, chest radiography | ||
| Pregnancy: pregnancy test in women of childbearing age, with pelvic ultrasonography if ectopic pregnancy is suspected | ||
| Patient report of previous organic or functional gastrointestinal affliction | Chronic psychogenic vomiting | Electrolyte levels, further evaluation if organic cause is suspected |
| Projectile airsickness, may not be preceded past nausea | Intracranial disorders, increased intracranial force per unit area (besides associated with normal emesis) | Brain computed tomography |
| Regurgitation of undigested food | Achalasia, esophageal stricture, Zenker diverticulum | Esophagogastroduodenoscopy, upper gastrointestinal barium study |
| Airsickness before breakfast | Alcohol ingestion, increased intracranial pressure, pregnancy, uremia | Increased intracranial force per unit area: brain computed tomography |
| Pregnancy: pregnancy exam in women of childbearing age, with pelvic ultrasonography if ectopic pregnancy is suspected | ||
| Uremia: renal role testing, electrolyte levels | ||
| Airsickness during or shortly after meals | Anorexia, bulimia | Electrolyte levels |
| Vomiting partly digested food or chyme several hours after meals | Gastric outlet obstruction (no bile), gastroparesis | Obstruction: abdominal radiography |
[Source 6) ]
Projectile vomiting in adults diagnosis
Well-nigh weather condition can be diagnosed by findings from the history and physical examination. Diagnostic testing may exist warranted in patients with signs of significant dehydration (eastward.g., decreased urine output, skin tenting, dry out mucous membranes), signs of acidosis caused by diabetic ketoacidosis or another underlying disorder (e.g., markedly increased respiratory rate, fruity scent to jiff, contradistinct mental status), severe abdominal hurting or amplification, hematochezia, jaundice, melena, severe headache, urinary tract infection symptoms, abdominal hurting relieved past vomiting, hematemesis, or feculent airsickness seven) .
Figure 3. Evaluation of Nausea and Airsickness in Adults
[Source 8) ]
Imaging tests
Abdominal radiography is helpful in detecting bowel obstructions and kidney stones 9) . Computed tomography of the belly is useful for detecting infections (eastward.g., appendicitis, cholecystitis) and for additional testing for bowel obstruction and kidney stones that are non detected on radiography.24 In adults, abdominal radiography combined with clinical test and laboratory analysis (complete claret count and bones metabolic panel) is useful for predicting the need for urgent intervention in the first 24 hours of illness (sensitivity = 56%; specificity = 81%) 10) .
Right upper-quadrant ultrasonography is used to evaluate for gallstones. Hepatobiliary iminodiacetic acid scans can determine whether delayed gallbladder emptying is the cause of nausea and intestinal hurting when initial ultrasonography is negative.
Migraine should be diagnosed in patients who accept headaches with at least four of the following characteristics: pulsatile quality, elapsing of iv to 72 hours, unilateral location, nausea or vomiting, and disabling intensity 11) . Cluster-type headaches, headaches with abnormal neurologic findings, undefined headaches, and headaches aggravated by exertion or the Valsalva maneuver are more than likely to accept associated intracranial pathology 12) . Computed tomography or magnetic resonance imaging of the brain should be ordered for patients with these symptoms, and in those with other aberrant neurologic signs or symptoms.
References [ + ]
Source: https://healthjade.com/projectile-vomiting/
0 Response to "What Does It Mean When a Baby Projectile Vomits"
Post a Comment